Article: Summer 2026
The ACOOG Consult
Breast Health in Obstetrics and Gynecology: A Practical Guide to Screening, Imaging, and the Symptomatic Breast
American College of Osteopathic Obstetricians and Gynecologists
Learning Objectives
After reading this article, the obstetrician-gynecologist will be able to:
Apply current age- and risk-based breast cancer screening recommendations to average-risk and higher-risk patients.
Differentiate physiologic from pathologic breast findings and select age-appropriate diagnostic imaging for a palpable mass, nipple discharge, and skin changes.
Assess hereditary breast cancer risk using family history and validated models, and coordinate referral for genetic counseling and supplemental magnetic resonance imaging when indicated.
Interpret Breast Imaging Reporting and Data System (BI-RADS) categories and manage follow-up and referral pathways that close the loop on abnormal results.
Introduction
Breast cancer is the most commonly diagnosed cancer in American women and the second leading cause of cancer death among them (American College of Obstetricians and Gynecologists [ACOG], 2017). Obstetrician-gynecologists examine breasts more often than any other physician group because they care for women across the reproductive years and into midlife. For many patients, the obstetrician-gynecologist is the one physician who performs a breast risk assessment, orders screening, and triages a new symptom. Strong breast health practice rests on four skills: stratifying risk, ordering the correct screening study at the correct age, evaluating symptoms with age-appropriate imaging, and closing the loop on abnormal results. This article reviews each skill and the current evidence behind it.
The Obstetrician-Gynecologist's Role in Breast Health
Obstetrician-gynecologists hold three core responsibilities. First, they assess each patient's risk early enough to act on it, ideally by age 25 to 30. Second, they refer patients for the right screening study and interval. Third, they evaluate new symptoms and coordinate the diagnostic workup with radiology, breast surgery, oncology, genetics, and primary care. Definitive diagnosis and treatment sit with breast specialists, so timely and well-documented referral protects patients and reduces delay.
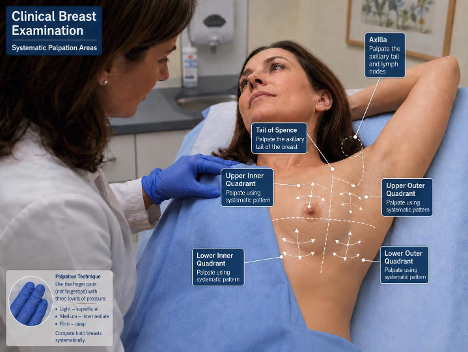
Clinical Breast Examination and Breast Self-Awareness
Routine breast self-examination no longer earns a recommendation for average-risk women. Encourage breast self-awareness instead, meaning familiarity with the normal look and feel of one's own breasts and prompt reporting of any change (ACOG, 2017). Clinical breast examination holds a more nuanced position. ACOG supports offering a screening clinical breast examination every one to three years for average-risk women aged 25 to 39, and annually from age 40, within a shared decision-making conversation (ACOG, 2017). The U.S. Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against clinical breast examination (U.S. Preventive Services Task Force [USPSTF], 2024), and the American Cancer Society no longer endorses it for average-risk women (Oeffinger et al., 2015). Make sure to document the discussion and the patient's choice.
Screening the Average-Risk Patient
Major United States organizations now converge on age 40 as the start of screening mammography for average-risk women. ACOG recommends beginning at age 40 and screening every one or two years through shared decision-making (ACOG, 2024). The USPSTF recommends mammography every other year from age 40 through 74, a grade B recommendation (USPSTF, 2024). The American College of Radiology (ACR) and the American Cancer Society support annual mammography beginning at age 40 (Monticciolo et al., 2023; Oeffinger et al., 2015).
The interval question, annual versus biennial, remains the main point of difference. Annual screening detects more cancers earlier at the cost of more false positives and recalls. Biennial screening reduces those harms with a small tradeoff in early detection. Match the interval to the patient's risk and preferences, and record the rationale. For older patients, continue screening while life expectancy reaches at least ten years and the patient values it. The USPSTF cites insufficient evidence beyond age 74, so individualize decisions for women 75 and older based on health status (USPSTF, 2024).
Assess risk before symptoms appear. ACR and the Society of Breast Imaging recommend a formal breast cancer risk assessment for every woman by age 25 (Monticciolo et al., 2023). Use a validated model such as Tyrer-Cuzick (IBIS), Gail, or BRCAPRO to identify patients who need earlier or supplemental screening.
Table 1. Screening by Risk Tier
| Risk Tier | Who Qualifies | Recommended Screening | Start Age and Interval |
|---|---|---|---|
| Average risk | No personal or strong family history, no high-risk gene variant, no prior chest radiation, lifetime risk below 15 percent | Mammography or digital breast tomosynthesis | Age 40; every 1 to 2 years |
| Intermediate risk | Personal history of breast cancer, lobular neoplasia, atypical hyperplasia, or 15 to 20 percent lifetime risk | Mammography; consider supplemental magnetic resonance imaging case by case | Individualized; annual mammography |
| High risk | BRCA1 or BRCA2 carrier or untested first-degree relative, other high-penetrance variant, chest radiation ages 10 to 30, or 20 percent or greater lifetime risk | Mammography plus annual breast magnetic resonance imaging | Magnetic resonance imaging ages 25 to 30; mammography phased in ages 25 to 40 |
Note. Sources: ACOG (2024); Monticciolo et al. (2023); U.S. Preventive Services Task Force (2024).
Identifying and Screening the Higher-Risk Patient
A lifetime breast cancer risk of 20 percent or greater, calculated with a model weighted toward family history, defines the high-risk group eligible for supplemental screening. Add annual breast magnetic resonance imaging (MRI) to mammography for these patients. Other high-risk groups include known BRCA1 or BRCA2 carriers and their untested first-degree relatives, carriers of other high-penetrance variants, and women who received chest radiation between ages 10 and 30. For these patients, annual MRI starts as early as ages 25 to 30, with annual mammography phased in between ages 25 and 40 depending on the type of risk. Women with a personal history of breast cancer plus dense tissue, and women diagnosed before age 50, also benefit from supplemental MRI. When MRI is not possible, contrast-enhanced mammography serves as the alternative (Monticciolo et al., 2023).
Refer for genetic counseling when the history raises concern. Red flags include breast cancer before age 50, ovarian cancer at any age, male breast cancer, triple-negative breast cancer before age 60, multiple affected relatives on the same side of the family, a known pathogenic variant in a relative, or Ashkenazi Jewish ancestry paired with breast or ovarian cancer history. A five-year Gail risk of 1.7 percent or higher opens a discussion of risk-reducing medication such as tamoxifen or an aromatase inhibitor (National Comprehensive Cancer Network [NCCN], 2025).
Address breast density directly. Dense tissue raises breast cancer risk and lowers mammographic sensitivity. Since September 2024, the U.S. Food and Drug Administration requires mammography facilities to notify patients of their breast density (U.S. Food and Drug Administration [FDA], 2024). Discuss supplemental screening individually. Evidence on routine supplemental ultrasound or MRI for dense breasts alone remains insufficient for a blanket recommendation, so weigh the patient's overall risk (USPSTF, 2024).
Choosing the Right Imaging Study
Each modality fills a defined role. Mammography and tomosynthesis anchor screening. Ultrasound targets symptoms and supplements screening in selected patients. MRI carries the highest sensitivity and serves high-risk surveillance and problem-solving (Monticciolo et al., 2023).
Table 2. Breast Imaging Modalities at a Glance
| Modality | Primary Role | Strengths | Limitations |
|---|---|---|---|
| Mammography / tomosynthesis | First-line screening and diagnostic imaging from age 40 | Proven mortality reduction; detects microcalcifications; tomosynthesis lowers recalls | Lower sensitivity in dense tissue; uses ionizing radiation |
| Ultrasound | Targeted evaluation of a palpable mass; first-line under age 30; supplemental in dense breasts | No radiation; distinguishes cystic from solid; safe in pregnancy | Operator dependent; not a standalone screening tool |
| Magnetic resonance imaging | Annual surveillance for high-risk patients; problem-solving | Highest sensitivity; no radiation | Lower specificity; cost and access; gadolinium contrast |
| Contrast-enhanced mammography | Alternative supplemental study when MRI is unavailable or contraindicated | Higher sensitivity than mammography alone; faster and lower cost than MRI | Iodinated contrast; less widely available |
Note. Source: Monticciolo et al. (2023).
Evaluating Common Breast Complaints
Palpable mass. Image a palpable mass by age. Under 30, start with ultrasound. From 30 to 39, ultrasound, diagnostic mammography, and tomosynthesis all apply, often together. At 40 and older, start with diagnostic mammography and tomosynthesis and add targeted ultrasound. A clinically suspicious, dominant, or persistent mass warrants tissue diagnosis even when imaging reads benign. Negative imaging does not overrule a concerning examination (Expert Panel on Breast Imaging, 2022b).
Nipple discharge. Separate physiologic from pathologic discharge. Physiologic discharge is bilateral, arises from multiple ducts, appears only with expression, and looks milky, green, or yellow. Reassure, and evaluate galactorrhea with a pregnancy test, prolactin, and thyroid-stimulating hormone. Pathologic discharge is unilateral, arises from a single duct, occurs spontaneously, and looks bloody, serous, or clear. Pathologic discharge needs imaging. US and Diagnostic Mammogram are indicated first, but most patients will require breast MRI for further evaluation. Underlying cancer accounts for roughly 5 to 20 percent of pathologic discharge, so persistent symptoms with negative imaging still warrant surgical referral for duct excision (Expert Panel on Breast Imaging, 2022a).
Breast pain. Mastalgia rarely signals cancer. Classify pain as cyclic or noncyclic. Reassure most patients, treat with supportive measures, and reserve imaging for focal, persistent, or unilateral pain, or pain paired with another finding.
Skin and nipple changes. Treat skin and nipple changes as red flags. Skin thickening, peau d'orange, nipple retraction, and an eczematous nipple point toward malignancy, including inflammatory breast cancer and Paget disease. A presumed mastitis in a nonlactating woman that fails to clear with antibiotics needs biopsy to exclude inflammatory breast cancer.
Lactation-related concerns. Pregnancy and lactation do not block needed imaging. Ultrasound evaluates most pregnancy- and lactation-related complaints first, and diagnostic mammography stays safe with abdominal shielding when indicated. Evaluate mastitis, abscess, and galactocele on their merits, and image a discrete mass that persists despite treatment. Pregnancy-associated breast cancer hides behind assumptions of benign change, so keep a low threshold for ultrasound and biopsy.
Table 3. Initial Imaging for the Symptomatic Breast, by Age
| Age Group | Palpable Mass | Pathologic Nipple Discharge |
|---|---|---|
| Under 30 | Ultrasound first; add mammography if findings are suspicious or risk is elevated | Ultrasound first; add mammography if findings are suspicious or risk is elevated |
| 30 to 39 | Ultrasound and diagnostic mammography or tomosynthesis, often combined | Ultrasound or mammography by institutional preference |
| 40 and older | Diagnostic mammography and tomosynthesis, plus targeted ultrasound | Diagnostic mammography or tomosynthesis, plus ultrasound |
Note. Sources: Expert Panel on Breast Imaging (2022a, 2022b).
Reading and Acting on Abnormal Imaging
The Breast Imaging Reporting and Data System (BI-RADS) standardizes radiology reports and drives the next step. The obstetrician-gynecologist confirms the loop closes. Track every BI-RADS 0, 3, 4, and 5 result until it resolves.
Table 4. BI-RADS Categories and Management
| Category | Assessment | Likelihood of Malignancy | Management |
|---|---|---|---|
| 0 | Incomplete | Not applicable | Additional imaging or prior-film comparison before a final category |
| 1 | Negative | ~0% | Routine screening |
| 2 | Benign finding | ~0% | Routine screening |
| 3 | Probably benign | >0% to ≤2% | Short-interval follow-up imaging (6, 12, and 24 months) |
| 4 | Suspicious | 2%–94% (overall) | Image-guided core needle biopsy |
| 4A | Low suspicion | 2%–10% | Tissue diagnosis |
| 4B | Moderate suspicion | >10%–50% | Tissue diagnosis |
| 4C | High suspicion | >50%–95% | Tissue diagnosis; repeat biopsy if benign |
| 5 | Highly suggestive of malignancy | ≥95% | Tissue biopsy and oncology coordination |
| 6 | Known biopsy-proven malignancy | 100% (confirmed) | Definitive treatment planning; see NCCN Breast Cancer Guidelines |
Note. Categories follow the American College of Radiology Breast Imaging Reporting and Data System (BI-RADS) Atlas.
Documentation, Counseling, and Referral Pathways
Document the risk assessment, breast density, examination findings, the imaging ordered, the BI-RADS category, the follow-up plan, and every referral. Record the shared decision-making for start age and interval. Build standing relationships with breast imaging, breast surgery, medical and surgical oncology, and genetic counseling. A short referral checklist inside the chart keeps abnormal results from slipping through the cracks.
Clinical Pearls for a Busy Practice
Run a formal risk assessment by age 25 to 30. Do not wait for symptoms to prompt it.
A clinically suspicious mass needs a biopsy even when imaging reads benign. The examination drives the decision.
Unilateral, spontaneous, single-duct, bloody discharge needs a full workup and surgical referral, even with a normal mammogram.
Antibiotic-refractory breast erythema in a nonlactating woman points to inflammatory breast cancer until biopsy proves otherwise.
Pregnancy and lactation are not reasons to delay needed imaging. Ultrasound comes first and is safe.
Document the interval and start-age decision as a shared one. The note protects the patient and the practice.
Areas of Evolving Guidance
Screening interval. ACR and the American Cancer Society favor annual mammography; the USPSTF favors biennial. The choice turns on how a patient weighs earlier detection against false positives (Monticciolo et al., 2023; USPSTF, 2024).
Supplemental screening for dense breasts. The FDA now mandates density notification, yet the evidence for routine supplemental ultrasound or MRI based on density alone remains insufficient for a universal recommendation (U.S. Food and Drug Administration, 2024; USPSTF, 2024).
Clinical breast examination. ACOG offers it within shared decision-making, while the USPSTF and the American Cancer Society deemphasize it for average-risk women (ACOG, 2017; USPSTF, 2024).
Stopping age. The USPSTF stops at 74 for lack of evidence; ACOG supports continuing while life expectancy reaches at least ten years (USPSTF, 2024; ACOG, 2024).
Emerging tools. Abbreviated MRI and contrast-enhanced mammography show promise as supplemental studies and are entering practice as access grows (Monticciolo et al., 2023).
References
American College of Obstetricians and Gynecologists. (2017). Breast cancer risk assessment and screening in average-risk women (Practice Bulletin No. 179). Obstetrics & Gynecology, 130(1), e1–e16. (Reaffirmed 2021)
American College of Obstetricians and Gynecologists. (2024, October). Updated recommendation on when to begin breast cancer screening mammography. acog.org
Expert Panel on Breast Imaging. (2022a). ACR Appropriateness Criteria: Evaluation of nipple discharge (2022 update). American College of Radiology.
Expert Panel on Breast Imaging. (2022b). ACR Appropriateness Criteria: Palpable breast masses (2022 update). American College of Radiology.
Monticciolo, D. L., Newell, M. S., Moy, L., Lee, C. S., & Destounis, S. V. (2023). Breast cancer screening for women at higher-than-average risk: Updated recommendations from the ACR. Journal of the American College of Radiology, 20(9), 902–914.
National Comprehensive Cancer Network. (2025). NCCN clinical practice guidelines in oncology: Breast cancer screening and diagnosis. nccn.org
Oeffinger, K. C., Fontham, E. T. H., Etzioni, R., Herzig, A., Michaelson, J. S., Shih, Y. C. T., Walter, L. C., Church, T. R., Flowers, C. R., LaMonte, S. J., Wolf, A. M. D., DeSantis, C., Lortet-Tieulent, J., Andrews, K., Manassaram-Baptiste, D., Saslow, D., Smith, R. A., Brawley, O. W., & Wender, R. (2015). Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA, 314(15), 1599–1614.
U.S. Food and Drug Administration. (2024). Mammography Quality Standards Act final rule: Reporting of breast density. fda.gov
U.S. Preventive Services Task Force. (2024). Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. JAMA, 331(22), 1918–1930.
Prepared as original CME content for ACOOG. All clinical recommendations rest on evidence accepted within the medical profession. Content is free of commercial bias and contains no copyrighted third-party figures.